A 25-year-old, tooth 36 in severe pain, saved in a single visit — Mr. Ayaan's story.
Mr. Ayaan came to our Engineers Town clinic with the most painful tooth in the most-loaded position in the mouth — the lower-left first molar, tooth 36, with severe spontaneous pain and lingering thermal sensitivity that had been disturbing his sleep for five days. This is the case file for the single-visit root canal that resolved his symptoms in one appointment and preserved a tooth that would otherwise have been heading toward extraction.
 BeforeAfter
BeforeAfterThe most-loaded tooth in the mouth. The most-rewarded to save.
Tooth 36 — the lower left first molar — is the workhorse of the chewing cycle. When it develops pulpal pathology, the case is one of the most urgent and most worth saving in routine endodontics.
Mr. Ayaan came in to our clinic on a busy weekday morning. He is 25 years old, working in IT, and a patient who had spent five days managing a progressively worse pain in his lower left side. The pain had escalated to the point that he could no longer sleep through the night without analgesics, and his work was being affected. He had been taking ibuprofen every four hours and the relief was diminishing with each dose.
The clinical picture pointed to a single tooth. Severe spontaneous pain that he could localise precisely to the lower left first molar — tooth 36. Sharp, lingering thermal sensitivity to both hot and cold stimuli. Tenderness on vertical percussion of the affected tooth. Localised swelling and gentle tenderness on palpation of the gum overlying the root. All consistent with one diagnosis: symptomatic irreversible pulpitis with early peri-apical involvement.
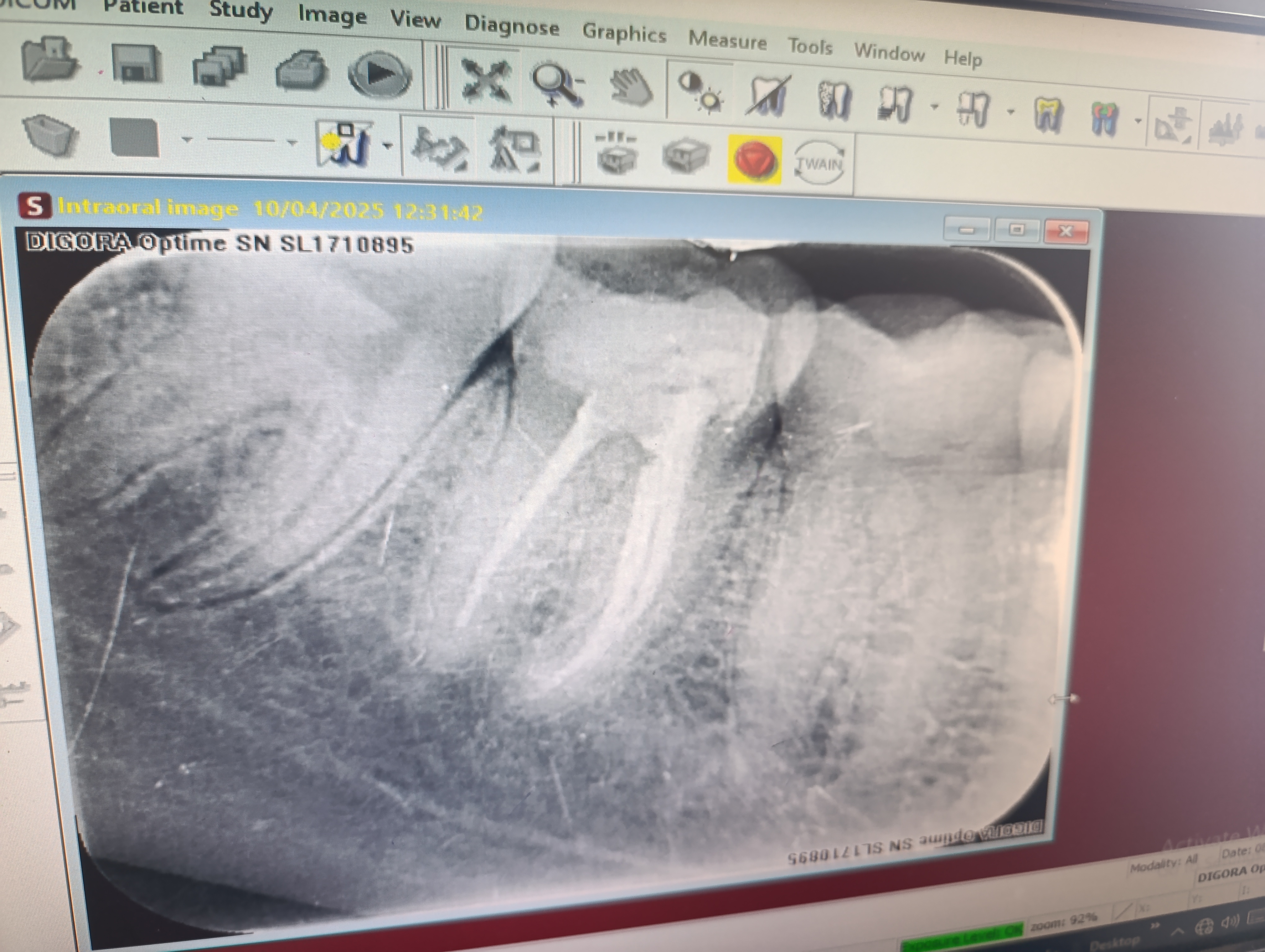
The clinical and radiographic workup took 30 minutes. We performed cold and percussion tests on tooth 36 and the two adjacent teeth — the response was sharp and lingering on 36, clean on the neighbours. We took a periapical X-ray that confirmed a deep carious lesion reaching close to the pulp chamber and a slight widening of the periodontal ligament space at the root tip — the early radiographic sign of peri-apical involvement.
We walked Mr. Ayaan through what we had found and the options. Option one: a same-day root canal, given that he was already in significant pain and was comfortable with our anaesthesia plan. Option two: emergency pain control today, definitive treatment in two days. Option three: extraction, with subsequent planning for an implant or bridge. We discussed the trade-offs for each. He chose option one. He was already off work, he had a long-term partner who could drive him home, and he wanted the case resolved that day.
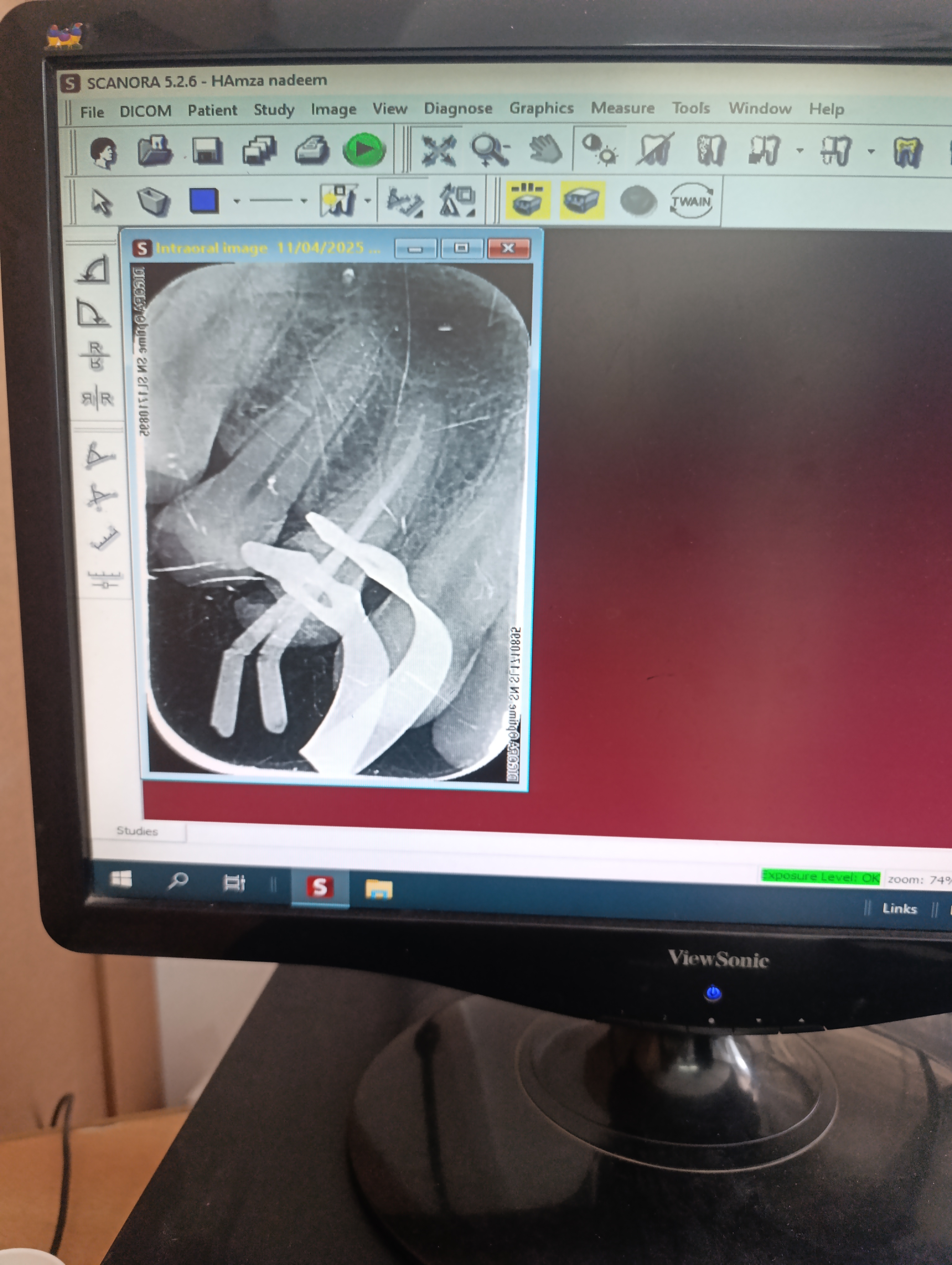
We administered an inferior alveolar nerve block with 4% articaine, gave it ten minutes to establish complete anaesthesia, and proceeded with the root canal in a single 2-hour session. By the time he left the clinic, the four canals of tooth 36 were cleaned, shaped, dried and obturated. The access cavity was sealed with a composite restoration. The post-obturation X-ray confirmed complete fill to the working length in all four canals. He was scheduled for a crown appointment at the 7-week mark.
He messaged on WhatsApp later that evening to confirm he had eaten a soft dinner on the opposite side and the pain that had been keeping him awake for five nights was completely gone.
A few details of this case are worth describing more fully because they explain why the lower first molar (tooth 36 in the FDI numbering) is one of the most rewarding teeth in the mouth to save with endodontic therapy. The tooth has four canals — two mesial canals running through the front root and two distal canals running through the back root — and complete cleaning of all four is essential to long-term success. The mesial canals frequently have a mild apical curvature that requires careful negotiation with size 10 K-files before the rotary instruments are introduced. We located all four canal orifices under magnification, negotiated the mesial curvature with patience, and instrumented each canal to its working length using a sequence of rotary nickel-titanium files.
The other technical decision worth recording is the choice to perform single-visit endodontics rather than splitting the work across two appointments. For decades, the convention in endodontics was to treat the canals in one visit and place an intracanal calcium-hydroxide medication, then return after one or two weeks to obturate. The reasoning was that the medication would continue to disinfect the canals during the interval. The contemporary published evidence does not support a meaningful advantage for that two-visit protocol in cases without acute infection. Single-visit endodontics with rigorous sodium hypochlorite irrigation has equivalent five-year success rates. The advantages of single-visit are real: the canals are obturated while at their cleanest state, the patient does not return for a second appointment, and the access cavity is permanently sealed without the risk of inter-appointment coronal leakage. Mr. Ayaan's case fit the single-visit criteria perfectly — no acute abscess, healthy patient, and a clear preference for finishing the procedure in one sitting.
The post-obturation X-ray we took at the end of the procedure showed gutta-percha fully extending to within 0.5 mm of the radiographic apex in all four canals, with no voids visible in the obturation material and no extrusion of sealer beyond the apex. This is the radiographic signature of a well-performed root canal and is one of the most reliable predictors of long-term success. The X-ray was sent to him by WhatsApp later that evening so he could share it with his family. Patients almost always find it reassuring to see the “after” image of their treated tooth — it makes the abstract clinical concept of a sealed canal feel tangible.
The plan from here was straightforward and discussed before he left: a one-week restoration review, a crown preparation at the seven-week mark, the final zirconia crown two weeks after that, and a six-month peri-apical X-ray review. He paid the all-inclusive fee for the root canal at the reception desk on the way out and booked the crown appointment in the calendar before leaving. The case was, from his perspective, complete in one afternoon. The follow-ups were maintenance.
Four findings, all consistent with one diagnosis.
When the clinical, radiographic and symptomatic findings all point to the same tooth and the same diagnosis, the case becomes straightforward to plan and predictable to execute.
Tooth 36 — lower left first molar — severely symptomatic
When Mr. Ayaan came in, he was able to point precisely to the affected tooth — the lower left first molar, tooth 36 in the FDI numbering system. This is the most-loaded molar in the mouth — the workhorse of the chewing cycle — and it is one of the most commonly affected teeth by adult-onset caries because of its complex occlusal anatomy and its position deep in the arch. The tooth was tender to vertical percussion, tender to digital palpation of the adjacent gum, and produced a sharp, lingering response to a cold stimulus. The signs were unambiguous.
Localised swelling and tenderness at the gum margin
The gum overlying the root of tooth 36 was visibly slightly swollen and tender to gentle palpation. There was no frank abscess pointing to the surface — no fluctuation, no draining sinus — but the soft tissue inflammation was already extending out from the apex of the tooth into the surrounding bone and gum. Catching the case at this early stage of peri-apical involvement, before any abscess formation, makes the root canal treatment significantly more straightforward.
Severe thermal sensitivity — both hot and cold
Mr. Ayaan described a textbook pattern of thermal sensitivity. Cold drinks produced an immediate sharp pain that lingered for thirty to sixty seconds after the stimulus was removed. Hot tea was even worse — the pain peaked sharply and continued for several minutes. The pattern of lingering response to thermal stimuli is the single most informative symptom in distinguishing irreversible pulpitis from reversible pulpitis. Reversible cases resolve within seconds; irreversible cases linger for tens of seconds to minutes.
Dependence on painkillers for daily function
Like many patients who reach this stage, Mr. Ayaan had been taking over-the-counter analgesics — ibuprofen and paracetamol — every four to six hours for the previous five days. He had reached the maximum daily dose and was no longer getting full relief. The pain had begun to disturb his sleep. The escalating analgesic requirement, the spontaneous pain, and the lingering thermal sensitivity together confirmed that the case was firmly into irreversible pulpitis territory and required definitive endodontic therapy.
Four phases. All in one 2-hour single-visit appointment.
Single-visit endodontics is appropriate for a case with no acute abscess and a healthy patient who is already comfortable with our anaesthesia plan. Mr. Ayaan met both criteria.
Diagnostic workup and pain control
Mr. Ayaan came in with a level of pain that made full clinical examination uncomfortable until we provided immediate anaesthesia. We administered an inferior alveolar nerve block with 4% articaine, which gave complete numbness of the lower left quadrant within ten minutes. Once he was comfortable, we performed cold and percussion tests on tooth 36 and the neighbouring teeth, took a periapical X-ray, and confirmed the diagnosis. With the workup complete, we could now decide whether to proceed with treatment the same day or to provide overnight relief.
Visit 1 · ~ 40 minAccess cavity preparation and pulp extirpation
Because the anaesthesia was already established and the patient was tolerating it well, we proceeded directly to the endodontic phase the same visit. We placed a rubber dam over tooth 36, prepared the access cavity through the occlusal surface, and located the four canal orifices of the lower first molar — two mesial, two distal. The pulp tissue was visibly inflamed, confirming the irreversible-pulpitis diagnosis intra-operatively. We removed the inflamed pulp tissue and irrigated the chamber with sodium hypochlorite.
Visit 1 · ~ 50 min (same appointment)Canal cleaning, shaping and obturation
Using a combination of hand files and rotary nickel-titanium instruments, we cleaned and shaped all four canals to their working length, which was confirmed in real time by an electronic apex locator. We irrigated repeatedly with sodium hypochlorite between every pass and finished with an EDTA rinse to remove the smear layer. The canals were dried with sterile paper points and obturated with gutta-percha and bioceramic sealer using a warm vertical compaction technique. A post-obturation X-ray confirmed complete fill to the working length in all four canals.
Visit 1 · ~ 70 min (same appointment)Post-endodontic restoration and recommendation for a crown
The access cavity was sealed with a glass-ionomer base and a composite resin restoration. Because tooth 36 is the most heavily loaded tooth in the lower arch and Mr. Ayaan is a young adult with many decades of chewing ahead, we discussed and strongly recommended a crown to be placed 6 to 8 weeks after the root canal. A crown distributes chewing forces across the cusps and prevents the slow vertical fracture that can otherwise develop in a non-vital posterior tooth under prolonged loading.
Visit 1 · ~ 20 min (same appointment)Same tooth. From inflamed pulp to sealed canals.
Drag the divider to compare the pre-operative radiograph with the post-obturation image taken at the end of the procedure.
BeforeAfterWhy single-visit endodontics works when it's done right.
Three conditions determine whether a root canal should be completed in a single visit or split across two. Mr. Ayaan's case met all three of the single-visit conditions.
No acute peri-apical abscess
When a tooth presents with frank pus, fluctuant swelling, or a draining sinus, the case usually benefits from a two-visit approach: open the canal for drainage at the first visit, leave it open temporarily, place an intracanal calcium-hydroxide medication, and complete the obturation at a second visit once the acute inflammation has resolved. For Mr. Ayaan, the peri-apical involvement was at the early stage with no abscess formation. Single-visit obturation was appropriate.
The patient is tolerating the anaesthesia and the duration well
A single-visit molar root canal is a 2-hour procedure with continuous anaesthesia and continuous rubber-dam isolation. The patient must be physically and psychologically tolerant of that duration. Some patients prefer to split the procedure across two shorter visits for comfort reasons; others — like Mr. Ayaan — prefer the single-visit completion. Both are valid, and the choice is the patient's.
The canal anatomy is being cleaned and shaped completely in one session
The biological success of a root canal depends on complete bacterial elimination from the canal system. That elimination depends on proper instrumentation and proper sodium hypochlorite irrigation, not on the number of visits. Single-visit endodontics with complete cleaning and shaping has the same success rate as two-visit endodontics with calcium-hydroxide medication, in the published comparative literature. The difference is convenience, not biology.
Five questions we hear at every molar root canal consult.
These are the worries we heard from Mr. Ayaan and the worries we hear from most adult patients facing a lower molar root canal. Tap any one to read the long answer.
Is a lower molar root canal more complicated than other teeth?+
Yes — modestly. The lower first molar has typically four canals (two mesial, two distal) compared to three canals in the upper molars and one or two in premolars. The mesial canals can have a curved anatomy that requires careful instrumentation with flexible nickel-titanium files. None of this is unusual, and none of it changes the success rate substantially — but it does mean the procedure usually takes longer than a single-canal anterior tooth or a two-canal premolar.
For Mr. Ayaan, the four canals of tooth 36 were located, cleaned, shaped and obturated in a single 2-hour appointment. The mesial canals had a mild apical curvature that we negotiated with hand files before completing the shaping with rotary instruments. The post-obturation X-ray confirmed complete fill to the working length in all four canals.
Do I really need a crown after a root canal on a back tooth?+
For lower molars, yes — the published evidence is clear that root-canal-treated lower molars without a crown have a substantially higher rate of vertical fracture compared to those protected with a crown. Tooth 36 in particular is the most-loaded tooth in the lower arch, and the loss of pulpal vitality combined with the loss of structural integrity from the access cavity makes it more vulnerable to fracture under chewing load.
The crown is typically placed 6 to 8 weeks after the root canal — long enough for any residual peri-apical inflammation to resolve, and for the patient to confirm that the tooth is comfortable on chewing. For Mr. Ayaan, the crown is scheduled and will be a zirconia crown matched to his other lower molars.
For an upper premolar like Mr. Aun's case, the situation is different — the chewing forces are lower and the risk of fracture is lower. A composite restoration may be adequate. For a lower first molar, a crown is the right protective measure.
Why was the pain so severe if it was just a cavity?+
A cavity that has reached the pulp produces inflammation in a confined space. The pulp inside a tooth sits in a hard chamber with no room to expand. As the inflammation builds, the pressure inside the chamber rises, which compresses the nerve fibres and produces severe pain. The pain is also amplified by the fact that pulpal nerves can only signal pain — they cannot signal mild discomfort or temperature accurately once the pulp is inflamed.
For Mr. Ayaan, the inflammation had been building for several days and the pressure inside the pulp chamber was high enough to produce constant pain that was no longer responding fully to over-the-counter analgesics. Opening the access cavity and removing the inflamed pulp tissue releases that pressure immediately, which is why patients almost always report a substantial relief during the procedure itself, before any of the cleaning and shaping has been completed.
How successful is root canal treatment? What is the failure rate?+
Published success rates for first-time root canal treatment on a molar with a healthy peri-apical bone are in the range of 90 to 95 percent at five-year follow-up, and 85 to 90 percent at ten-year follow-up. The failure modes are usually either persistent peri-apical inflammation that does not resolve, or a coronal leakage problem from a failed restoration on top of the root canal.
For Mr. Ayaan, the procedure was performed under rubber-dam isolation, with an electronic apex locator to confirm working length, with rotary nickel-titanium instrumentation, and with a warm vertical obturation. The post-operative X-ray confirmed complete fill of all four canals. The crown that will be placed at the 6-to-8-week mark will protect against coronal leakage. With this combination of measures, his case is at the upper end of the published success-rate range.
How do I take care of the tooth in the first few days after a root canal?+
The first 24 to 48 hours after a root canal are a brief recovery window during which the peri-apical bone settles after the disturbance of instrumentation. Most patients feel a mild tenderness on biting during this window — usually well-controlled with over-the-counter ibuprofen — and full normal sensation returns by the third or fourth day.
There are three specific things we asked Mr. Ayaan to do in the first 48 hours. First, avoid chewing on the treated side entirely — he was asked to chew on the right side only during this window. Second, take the prescribed five-day course of amoxicillin even if he felt fine. Third, message us on WhatsApp if anything felt unexpected, particularly any persistent throbbing pain, any new swelling, or any sensation that the tooth was “raised” relative to the others.
After the first 48 hours, normal chewing on soft foods on the treated side is fine, but he was asked to favour the other side for harder foods until the crown was placed at the 7-week mark. The temporary composite restoration we placed at the end of the root canal is functional but not as durable as the final crown will be, and biting directly into hard food during that window could chip or fracture the composite.
For oral hygiene, gentle brushing around the treated tooth from day one is encouraged. The gum overlying the root tip will be mildly tender for the first 7 to 10 days, and a soft-bristled brush used with light pressure is appropriate. Aggressive brushing in the recovery window can irritate the still-recovering peri-apical soft tissue and prolong the tenderness window.
What does it cost? Is it cheaper than an extraction plus implant?+
A root canal of a four-canal molar at our clinic is quoted in writing at consultation. The fee covers the diagnostic radiographs, the local anaesthesia, the rubber-dam isolation, the full endodontic instrumentation, the obturation, the post-endodontic composite restoration, and the immediate post-operative X-ray. There is no separate charge for the apex locator, the irrigation solutions, or the rotary instruments. The recommended crown is quoted and billed separately at the time of the crown visit.
A root canal plus crown is substantially cheaper than an extraction plus implant plus crown, and it preserves the natural tooth and its natural root. Even when the cost of the eventual crown is added, the total is typically less than half the cost of an implant-supported alternative.
For Mr. Ayaan, the root canal was completed within a single all-inclusive fee. The crown will be quoted at the crown appointment.
The follow-up visits.
A root canal on tooth 36 is followed by two scheduled appointments — the crown at 6 to 8 weeks, and a peri-apical X-ray review at six months to confirm the bone has healed completely.
He messaged on the second day post-treatment to confirm the pain had completely resolved, the swelling was reducing, and he had stopped taking analgesics. He was eating soft food on the opposite side and sleeping through the night again.
A short 10-minute visit to check the access restoration with articulating paper, percussion-test the tooth, and palpate the gum over the root. All tests clean. The composite restoration was sealed and well-contoured.
He returned for the planned crown work — tooth preparation, digital scan, and a chair-side acrylic temporary crown. The final zirconia crown was cemented two weeks later. The bite was balanced and the shade matched his other lower molars.
A fresh peri-apical X-ray confirmed full peri-apical bone healing. The slight widening of the periodontal ligament space visible pre-treatment had resolved. The crown was in place, sealed, and functioning normally.

Dr. Mian Momin Ahmad
“A four-canal molar root canal in a single visit is technically demanding but it is one of the most satisfying procedures in general practice when the case fits. The 25-year-old patient walks in suffering after five days of bad sleep, and walks out two hours later with the tooth saved, the pain gone, and a crown plan in place. Mr. Ayaan's case is exactly the kind of case that endodontic therapy was designed to handle.”
Six habits that protect a lower-molar root canal.
A lower first molar is the most-loaded tooth in the mouth. The aftercare reflects that — particularly the recommendation for a protective crown.
Avoid chewing on the treated side for two weeks
A root-canal-treated molar is functionally weaker than a vital molar for the first two weeks while the peri-apical bone fully resolves any residual inflammation. Mr. Ayaan was asked to chew exclusively on the right side for the first 14 days, and to favour the right side for soft foods for an additional month.
Schedule the crown within 6 to 8 weeks
For a lower molar, particularly the most-loaded tooth 36, a crown is strongly recommended within 6 to 8 weeks of completing the root canal. The crown protects the cusps from vertical fracture under chewing load and substantially extends the long-term service life of the tooth. Mr. Ayaan's crown appointment was booked at the end of the root canal visit.
Take the prescribed antibiotics as directed
A five-day course of amoxicillin was prescribed to address any residual peri-apical bacterial involvement. We asked him to complete the full course even if symptoms resolved earlier, which they did within 48 hours.
Brush gently around the treated tooth for the first week
The gum overlying the root of tooth 36 is recovering from peri-apical inflammation and is mildly tender for 7 to 10 days. A soft-bristled brush, used with light pressure, prevents further irritation while the gum heals.
Watch for any return of tenderness on biting
Properly treated root canals almost always heal without complication. In a small minority of cases, a residual infection can persist and produce a recurrence of tenderness or a small lump on the gum. The early warning sign is a sensation of the tooth being slightly raised. We asked Mr. Ayaan to flag any return of symptoms immediately.
Return for the six-month review and the crown placement
Two follow-up visits are scheduled — the crown placement at 6 to 8 weeks, and a peri-apical X-ray review at six months to confirm the bone around the root tips has fully healed. The image is compared against the post-operative X-ray taken on the day of treatment.
Tooth 36 is the most-saveable molar in the most-loaded position.
Many adults who develop severe pain in a lower back molar assume the case will end in extraction. With modern endodontics, the opposite is true for most cases caught at the irreversible-pulpitis stage. The tooth can be saved, the pain resolved, and a protective crown placed within two months.
Mr. Ayaan came in at day five — the right time. The case was a routine single-visit root canal. Waiting another two weeks would likely have moved it into the two-visit protocol territory.
More on molar root canals and crowns.
Severe pain in a lower molar? Call us — we see emergencies the same day.
We keep emergency slots for severe pain every day. The first visit will diagnose, give you pain relief, and either start the definitive treatment the same day or book it for the next morning. No pressure to commit to anything without a written quote.