An 18-year-old, severe premolar pain, and a root canal that saved the tooth — Mr. Aun's story.
Mr. Aun is an 18-year-old student who walked into our Engineers Town clinic as an emergency one weekday afternoon with visible facial swelling on the right side, severe spontaneous pain in a single upper tooth, and a description of symptoms that pointed almost immediately to one diagnosis. This is the case file for the two-visit root canal treatment that resolved the pain, drained the inflammation, and preserved his upper-right first premolar.
 Before
Before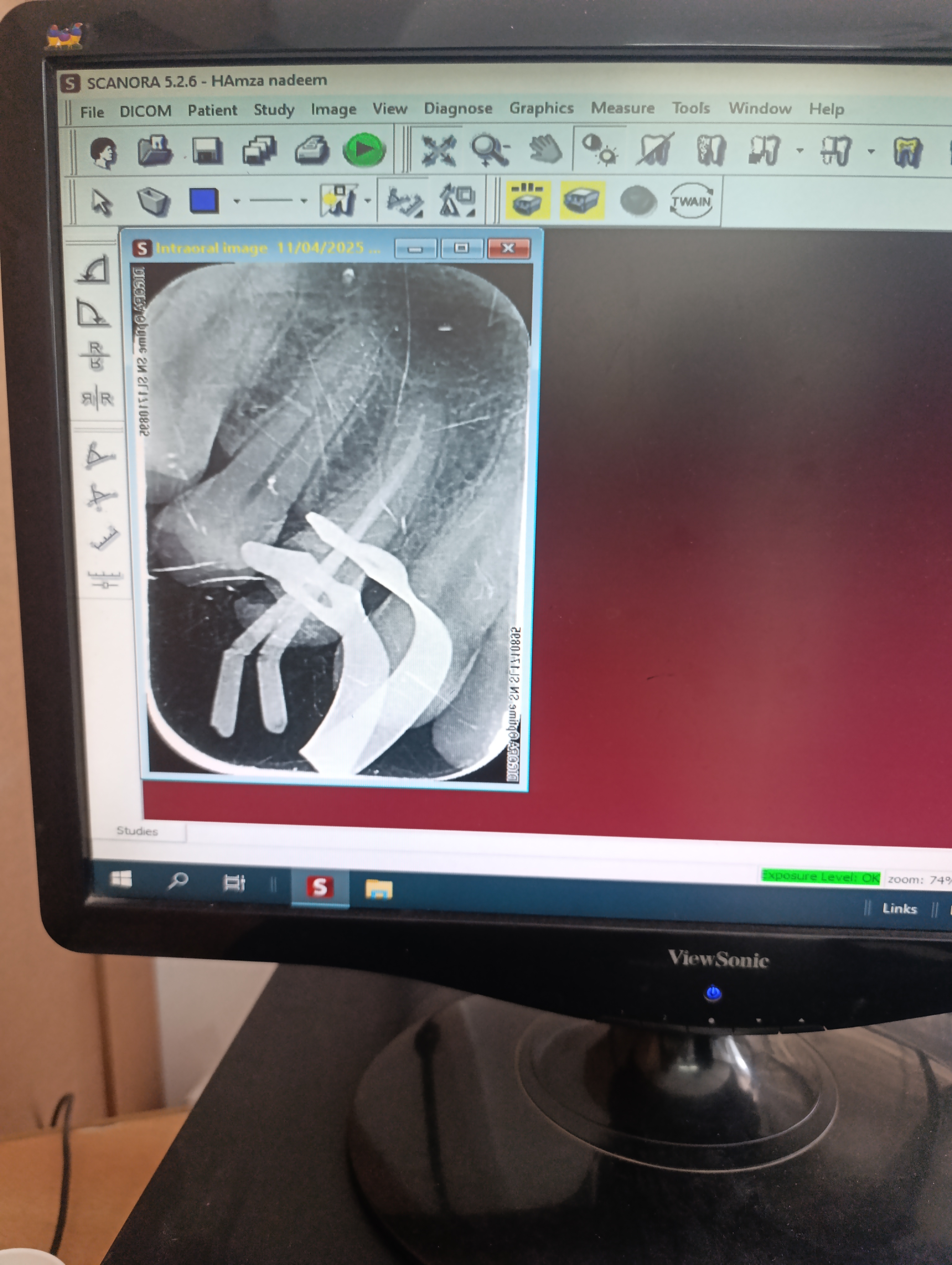 After
AfterAn emergency walk-in. A textbook diagnosis. A two-visit fix.
Severe spontaneous tooth pain with visible facial swelling in a young patient is one of the most common emergencies in general dental practice. The diagnostic pathway is well-established, and the treatment — done in the right order — is highly predictable.
Mr. Aun walked into our clinic just after 4 PM on a Thursday afternoon. He is 18 years old, a college student living at home with his parents, and he had been managing — with progressively less success — a severe pain in his upper-right side for about three days. The pain had escalated to the point that he could no longer concentrate in class, could not eat normally, and had been losing sleep. His mother had brought him in after he had taken his fourth dose of ibuprofen that day with diminishing effect.
The clinical picture was easy to read. Visible soft-tissue swelling on the upper-right cheek. Severe spontaneous pain that he could localise precisely to a single upper tooth. Pain made worse by hot drinks and very briefly relieved by holding cold water against the tooth. A history of escalating analgesic use over three days with diminishing relief. This combination of findings has essentially one diagnosis in an 18-year-old: symptomatic irreversible pulpitis, with early peri-apical involvement and adjacent soft-tissue inflammation.
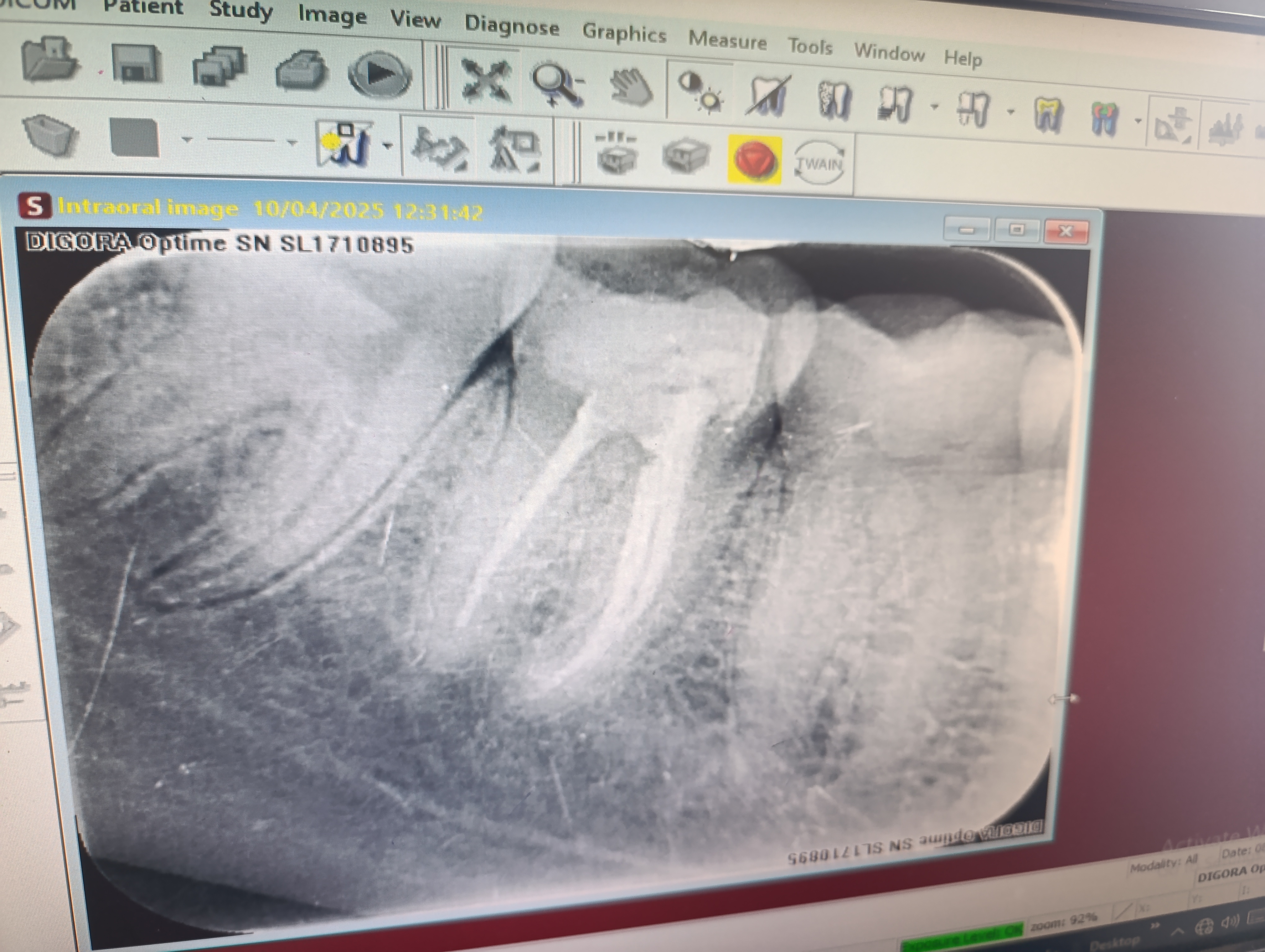
The diagnostic workup took 25 minutes. We took a peri-apical X-ray of the upper-right premolar region, which showed slight widening of the periodontal ligament space at the apex of tooth 14 — an early radiographic sign that the inflammation had begun to extend out through the apex into the bone. We performed a cold-stimulus test that produced a sharp, severely lingering response — the pain continued for over a minute after the stimulus was removed, which is the textbook signature of irreversible pulpitis. We performed vertical percussion testing that produced sharp tenderness on tooth 14 and nothing on the adjacent teeth.
The diagnosis was clear: irreversible pulpitis of tooth 14 with peri-apical involvement. The treatment was a root canal. The question was whether to start it the same afternoon or to provide emergency pain relief and start the definitive treatment the following morning when both of us would be fresh and the inflammation would have had a few hours to settle under antibiotics.
We chose the second approach. We administered a long-acting local anaesthetic block that took the pain away within ten minutes. We prescribed a five-day course of amoxicillin to address any bacterial involvement in the peri-apical bone, and a stronger anti-inflammatory for the overnight period. We booked the definitive treatment for 10 AM the following morning. We checked on him by WhatsApp at 9 PM that evening — he was comfortable, eating soft food, and the swelling had already reduced visibly.
The next morning he arrived on time, with the swelling about half the size it had been the previous afternoon. We numbed the quadrant, placed a rubber dam, and performed the root canal treatment in a single session lasting roughly two hours. By the time he left, the tooth was fully sealed, the obturation X-ray confirmed a complete fill, and the pain that had been keeping him awake for three nights was completely gone.
There is a detail of his case worth describing because it helps explain why we sometimes choose to delay the definitive treatment by 12 to 18 hours rather than starting it the same evening. Endodontic treatment performed on a tooth with significant peri-apical inflammation has a slightly higher rate of post-operative discomfort if the inflammation has not been allowed to settle first. Adding a brief period of antibiotics and anti-inflammatory medication, with the patient comfortable on a long-acting local anaesthetic block, lets the surrounding tissues become less reactive before instrumentation begins. The biological success of the case is no different — it is just the post-operative experience that is meaningfully better. For an 18-year-old who had been in severe pain for three days and was understandably frightened, that comfort difference was worth the overnight wait.
The instrumentation phase of the procedure deserves some explanation, because the technical detail is part of why modern root canals have a 90 to 95 percent success rate at five years. We used a sequence of rotary nickel-titanium instruments — a more flexible alloy than the stainless-steel files used in older techniques — which allowed us to negotiate the slightly curved apical anatomy of his premolar canals without instrument fracture. An electronic apex locator confirmed the working length of each canal in real time, replacing the older method of repeated radiographs and allowing us to instrument the canals to within 0.5 mm of the apex with high precision. The combination of these two technologies — flexible files and electronic apex location — is the reason a modern root canal can be completed in 90 minutes instead of the multi-visit protocols common a generation ago.
The irrigation protocol is the chemical core of the case. Between every mechanical instrumentation pass, we irrigated the canals with 3% sodium hypochlorite — the same active ingredient as household bleach but at a controlled, dental-grade concentration. Sodium hypochlorite dissolves residual pulp tissue, disrupts bacterial biofilms, and disinfects the dentinal tubules deep into the canal wall. We finished with an EDTA rinse to remove the smear layer created by mechanical instrumentation, which exposes fresh dentine and allows the sealer to bond to the canal walls directly. The total irrigation volume across the case is typically 30 to 40 ml — far more than most patients realise — and this volume is what gives the procedure its disinfection power.
By the end of the visit, the access cavity was sealed with a glass-ionomer base under a composite resin restoration. The bite was checked with articulating paper and balanced. Mr. Aun walked out to the reception desk, drank a glass of water, and went home with his mother. He messaged at 9 PM that evening to confirm he was about to eat soft food and the residual tenderness was already minimal. The procedure had saved a tooth that would otherwise have moved toward extraction within a few weeks.
Four findings, all pointing to the same diagnosis.
When the clinical findings, the radiographic findings, and the patient's symptomatic history all point to the same diagnosis, the case is straightforward. Mr. Aun's presentation was as clear as a root-canal indication gets.
Visible facial swelling on the upper-right side
When Mr. Aun walked into the consultation room, the swelling on the right side of his face was immediately visible — a soft, tender, slightly red enlargement of the cheek tissue overlying his upper-right maxillary region. The skin was warm to the touch but not hot. There was no fluctuation suggesting a frank abscess pointing to the surface yet. This kind of soft-tissue swelling around an upper premolar is a classic sign of an inflamed pulp in that tooth that has begun to extend into the surrounding bone and adjacent soft tissue.
Tooth 14 — the upper-right first premolar — was severely symptomatic
The pain Mr. Aun described was localised to a single tooth. He could point to it directly with one finger — an unusual precision that immediately narrows the diagnosis. The tooth in question was the upper-right first premolar (tooth 14 in the FDI numbering system). It was tender to vertical percussion (tapping the chewing surface), tender to palpation of the gum over the root tip, and produced a sharp, lingering response to a cold stimulus. The pain pattern he described — spontaneous, severe, increased by hot food and drinks, often requiring painkillers — fit the picture of symptomatic irreversible pulpitis with early peri-apical involvement.
Severe thermal sensitivity, particularly to heat
Mr. Aun described a particularly informative pattern: the pain was made worse by hot drinks, and (paradoxically) sometimes briefly relieved by holding cold water against the tooth. This combination — heat-aggravated, cold-relieved pain — is essentially pathognomonic of irreversible pulpitis with gas-producing bacterial activity inside the pulp chamber. The cold water briefly contracts the gases, providing transient relief; the heat expands them, producing severe pressure on the pulpal nerve fibres.
Reliance on painkillers for daily function
By the time he came to see us, Mr. Aun had been taking ibuprofen and paracetamol every 4 to 6 hours for several days. The painkillers were taking the edge off but not eliminating the pain entirely, and he had begun to need higher and more frequent doses to get the same relief. This pattern of escalating analgesic requirement, combined with the spontaneous and lingering nature of the pain, was further confirmation that the case had moved past reversible pulpitis into a stage where only definitive endodontic therapy would resolve it.
Four phases. Two visits across 24 hours.
The first visit was diagnosis and emergency pain control. The second visit, the next morning, was the definitive endodontic treatment performed in a single 2-hour session.
Diagnostic workup and emergency pain relief
Mr. Aun arrived as an emergency walk-in late one afternoon. We saw him within twenty minutes. The first task was to confirm the diagnosis and provide immediate pain relief — not to start the root canal that same day, but to make him comfortable enough to go home and return for definitive treatment the next morning. We took a periapical X-ray (showing the slight widening of the periodontal ligament at the root tip), performed cold and percussion tests, charted the surrounding gum, and gave him a long-acting local anaesthetic block that relieved the pain completely within ten minutes. We prescribed a course of amoxicillin and a stronger anti-inflammatory for the overnight gap.
Visit 1 · ~ 45 minAccess cavity preparation and pulp extirpation
The following morning he returned, comfortable, with the swelling already substantially reduced. We numbed the quadrant with a buccal and palatal infiltration, placed a rubber dam over tooth 14, and prepared the access cavity through the occlusal surface. The pulp chamber was visibly inflamed — a clear sign that the irreversible-pulpitis diagnosis had been correct. We carefully removed the inflamed pulp tissue (a step called pulp extirpation) using fine endodontic files and irrigated with sodium hypochlorite.
Visit 2 · ~ 60 minCleaning, shaping and apex location
Using a combination of hand files and rotary nickel-titanium files, we cleaned and shaped both root canals of the premolar to a standardised final dimension. An electronic apex locator confirmed the working length of each canal in real time. We irrigated repeatedly with sodium hypochlorite between every instrumentation pass to dissolve any remaining pulp tissue and disinfect the canal walls. A final EDTA rinse removed the smear layer and prepared the dentinal tubules for the obturation material.
Visit 2 · ~ 35 min (same appointment)Obturation and post-endodontic restoration
Once the canals were fully cleaned, shaped and dried with sterile paper points, we obturated them with gutta-percha and a bioceramic sealer using a warm vertical compaction technique. The access cavity was sealed with a glass-ionomer base, and a tooth-coloured composite resin was placed over the top to restore the occlusal anatomy. A post-operative periapical X-ray confirmed the obturation was complete to the working length with no voids visible.
Visit 2 · ~ 40 min (same appointment)Same tooth. Pre-operative pain. Post-operative seal.
Drag the divider across the photo to compare the pre-operative peri-apical X-ray with the post-obturation X-ray taken at the end of the second visit.
BeforeAfterWhy a root canal saves rather than destroys the tooth.
Three principles explain why endodontic treatment is one of the most reliable preservation procedures in modern dentistry, despite its reputation.
The pulp is replaceable; the tooth structure is not
The pulp inside a tooth is the soft tissue that provides nourishment and sensation during the developmental phase. Once a tooth is mature (typically by mid-adolescence), the pulp's biological role is largely complete. The hard tissue of the tooth — the enamel, dentine, and cementum — continues to function with or without a living pulp. Removing the inflamed pulp and replacing it with a sealed inert filling material allows the hard tooth structure to remain in service.
Sodium hypochlorite irrigation eliminates the bacterial source
The inflammation in irreversible pulpitis is driven by bacterial colonisation of the pulp tissue. The bacteria themselves cannot be removed mechanically because the canal walls are microscopic. Sodium hypochlorite irrigation, used between every instrumentation pass, dissolves residual pulp tissue, disrupts the bacterial biofilm, and disinfects the dentinal tubules. This is the chemical core of a successful root canal, and it is the reason properly treated cases do not relapse.
The obturation seals the canal against future bacterial leakage
Once the canal has been cleaned and shaped, it is filled with gutta-percha and a bioceramic sealer using a warm vertical compaction technique. The combination produces a three-dimensional seal that prevents any future bacterial leakage from the oral cavity into the peri-apical bone. The final post-endodontic restoration on top — composite, sometimes a crown — protects against leakage from the access cavity. The two seals together are what give the procedure its 15-to-20-year service life.
Five questions we hear at every emergency root-canal consult.
These are the worries we heard from Mr. Aun's family and the worries we hear from most young patients facing their first root canal. Tap any one to read the long answer.
Is a root canal painful? I've heard horror stories.+
The honest answer is: no — and the reason people associate root canals with pain is that they are often performed on teeth that are already in severe pain before the treatment begins. The procedure itself, done with proper local anaesthesia, is no more uncomfortable than a routine filling.
For Mr. Aun, the procedure was done under a buccal and palatal infiltration of articaine, which gave complete numbness for the full duration of the appointment. He felt pressure at certain stages — particularly during the access cavity preparation — but he reported no pain at any point. The pain he had been experiencing for several days before the appointment was completely resolved by the end of the visit.
The myth that root canals are painful comes from older techniques and from cases where the local anaesthesia was inadequate for the level of inflammation. With modern techniques and proper technique, the procedure is comfortable for the vast majority of patients.
Will the tooth become brittle and break later?+
This is a real concern and deserves an honest answer. A root-canal-treated tooth is more brittle than a vital tooth because the pulp is no longer providing internal hydration to the dentine. Over years, the tooth can become slightly more susceptible to fracture under heavy chewing load.
The protective measure for premolars and molars after endodontic treatment is a crown — a fitted cover that distributes chewing forces across the cusps and prevents vertical fractures. The recommendation for a crown depends on how much tooth structure remains after the root canal access and the original cavity. For Mr. Aun, the remaining structure was strong enough that the composite restoration was adequate. We will reassess at the six-month recall and recommend a crown if any signs of stress emerge.
For an upper premolar in particular, the risk of fracture is lower than for a posterior molar because the chewing forces are lower. Many premolars treated with adequate composite restoration last decades without needing a crown.
Why couldn't I just have the tooth extracted instead?+
Extraction is always an option, and we discussed it with Mr. Aun honestly at the diagnostic visit. There are two situations where extraction is the right choice: when the tooth is so badly damaged that it cannot be predictably restored, or when the patient has a strong personal preference for extraction and is aware of the consequences.
For Mr. Aun, the tooth was eminently restorable. The structural damage was confined to a discrete decay area; the remaining tooth structure was strong; and the surrounding bone was healthy enough to support the tooth after endodontic treatment. Removing a restorable natural tooth at 18 years of age means committing the patient to either a long-term gap, a bridge using the adjacent teeth as abutments, or an implant. None of those options is better than keeping the natural tooth when the natural tooth can be saved.
The principle is straightforward: when a natural tooth can be saved with a predictable procedure, saving it is almost always the better long-term decision than extracting it.
How long does the root canal treatment last?+
Properly performed root canal treatment on a sound abutment tooth with a good final restoration lasts 15 to 20 years in the published literature, and many cases last considerably longer. The single biggest determinant of how long the result lasts is the quality of the final restoration — how well the access cavity is sealed against bacterial leakage.
For Mr. Aun, the access cavity was sealed with a glass-ionomer base and a composite resin restoration. We will reassess the durability of this restoration at the six-month and twelve-month recalls. If the restoration shows any signs of marginal breakdown, we will replace it before any leakage can compromise the root canal seal.
With a well-sealed restoration and routine six-monthly recall, this tooth can serve him for the rest of his adult life. He is 18 now; we would expect the same tooth to be functioning normally when he is 40.
Why was the swelling so bad if it was just inside the tooth?+
The swelling Mr. Aun developed was the result of the pulpal inflammation extending out through the apex of the root and into the surrounding bone and soft tissue. The pulp inside the tooth is enclosed in a hard chamber with very little room to expand. When the pulp becomes inflamed, the pressure builds up because there is nowhere for the inflammation to go. Eventually it forces its way out through the apex of the root.
Once the inflammation is in the surrounding tissue, the body mounts a normal immune response — increased blood flow, white-cell infiltration, fluid accumulation. That is what produces the visible facial swelling. Treating the source — the inflamed pulp — by removing it from inside the tooth allows the body's natural healing response to resolve the surrounding tissue inflammation within days.
For Mr. Aun, the swelling had reduced substantially by the morning after the first emergency visit (with the antibiotics and pain control in place), and resolved completely within the first week after the definitive root canal treatment.
The follow-up visits.
A root canal is finished six months after obturation, once the bone around the root tip has fully healed and the restoration on top has been confirmed sealed. Here is how Mr. Aun's follow-up went.
He messaged on the second day post-treatment to confirm the swelling had resolved completely and he was eating normally on the opposite side. No new pain. Antibiotic course progressing normally.
A short 15-minute visit to check the access restoration, percussion-test the tooth, and palpate the gum over the root tip. No tenderness on either test. He had completed the antibiotic course and was no longer taking analgesics.
We took a fresh peri-apical X-ray and compared it with the post-obturation image from the day of treatment. The widening of the periodontal ligament space that had been visible pre-treatment was now fully resolved. The bone around the root tip looked normal in density and architecture. The composite restoration was intact with no marginal staining.

Dr. Mian Momin Ahmad
“Treating an 18-year-old emergency is one of the most rewarding situations in general practice. The patient comes in suffering, frightened, and convinced the tooth is lost. The diagnostic pathway is clear, the treatment is well-established, and the result is a young person leaving the clinic the next morning with the tooth saved and the pain completely resolved. The myth that a root canal is the same as losing the tooth is one of the most persistent in dentistry, and every successful case is a small piece of evidence against it.”
Six habits that protect a freshly treated root canal.
The most important window is the first two weeks. These six habits cover both the immediate healing phase and the long-term protection of the tooth.
Take the prescribed antibiotics and analgesics as directed
Mr. Aun was prescribed a five-day course of amoxicillin and a short course of ibuprofen. The antibiotics complete the eradication of any residual infection extending into the peri-apical bone; the anti-inflammatory addresses the residual swelling. We asked him to complete the full antibiotic course even if symptoms resolved earlier, which they did.
Avoid chewing on the affected side for two weeks
A root-canal-treated tooth is functionally weaker than a healthy tooth for the first two weeks while the surrounding bone fully resolves any residual inflammation. We asked him to chew on the opposite side for two weeks, and then to favour the opposite side for soft foods for another month.
Consider a crown if the tooth has lost significant structure
A tooth that has undergone endodontic treatment is more brittle than a vital tooth — the pulp is no longer providing internal hydration to the dentine. For a premolar that has lost significant structure, a crown placed 6 to 8 weeks after the root canal protects the cusps from fracture under chewing load. For Mr. Aun, the remaining tooth structure was strong enough that the composite restoration was adequate, but we will reassess at the six-month recall.
Brush gently around the treated tooth for the first week
The gum overlying the root tip is recovering from a period of inflammation and is mildly tender for the first 7 to 10 days. A soft-bristled brush, used with light pressure, prevents the gum from being further irritated while it heals.
Watch for any return of symptoms
Almost all properly treated root canals heal without complication. In a small minority of cases, a residual infection can persist and produce a recurrence of tenderness or swelling weeks or months later. The early warning signs are a return of tenderness on biting, a small lump on the gum near the root tip, or a sensation of the tooth being slightly "raised". We asked Mr. Aun to message immediately if any of these appeared.
Return for the six-month review
Every root canal patient at our clinic comes back at six months for a peri-apical X-ray to confirm the bone around the root tip has healed completely. The image is compared against the post-operative X-ray taken on the day of treatment. Twenty minutes, no charge for the review itself.
Severe spontaneous tooth pain is almost always a treatable diagnosis.
Many young patients put off seeing a dentist when they develop severe tooth pain because they assume the tooth will need to be extracted. The opposite is more often true. The earlier the patient comes in with severe pain, the more likely the tooth can be saved with a routine root canal. Waiting another week or two often does not change the treatment plan; it just extends the days of suffering for no clinical reason.
Mr. Aun came in at day three. The case was a routine two-visit root canal. Waiting another week would not have changed the treatment plan — it would only have added another week of pain.
More on root canals and pulpal disease.
More root canal cases.

Severe tooth pain right now? Call us — we see emergencies the same day.
We keep emergency slots open every day for severe pain and facial swelling. The first visit will diagnose, give you pain relief, and book the definitive treatment for the next available morning. No pressure to commit to anything without a written quote.